ISSN : 0975-3702
EISSN : 0975-9182

UJAGARE M.1, JADHAV R.2, BAWAL S.3, NAGDAWANE R.P.4, GANDHAM N.5, SHARMA M.6, DHUMAL P.7, JADHAV S.V.8*
1Department  of Microbiology, Pad. Dr. D.Y. Patil Medical College and Hospital Pimpri, Pune- 411018, MS, India.
2Department of Pediatrics, Pad. Dr. D.Y. Patil Medical College and Hospital Pimpri, Pune- 411018, MS, India.
3Department  of Microbiology, Pad. Dr. D.Y. Patil Medical College and Hospital Pimpri, Pune- 411018, MS, India.
4Department  of Microbiology, Pad. Dr. D.Y. Patil Medical College and Hospital Pimpri, Pune- 411018, MS, India.
5Department  of Microbiology, Pad. Dr. D.Y. Patil Medical College and Hospital Pimpri, Pune- 411018, MS, India.
6Department  of Microbiology, Pad. Dr. D.Y. Patil Medical College and Hospital Pimpri, Pune- 411018, MS, India.
7Department of Microbiology, Sancheti Hospital, Centre of Joint Replacement Surgery, Dhube Park, Shivaji Nagar, Pune- 411005, MS, India.
8Department  of Microbiology, Pad. Dr. D.Y. Patil Medical College and Hospital Pimpri, Pune- 411018, MS, India.
* Corresponding Author : patilsv78@gmail.com
Received : 03-10-2012 Accepted : 18-10-2012 Published : 06-12-2012
Volume : 4 Issue : 2 Pages : 94 - 99
Int J Parasitol Res 4.2 (2012):94-99
DOI : http://dx.doi.org/10.9735/0975-3702.4.2.94-99
Conflict of Interest : None declared
Introduction- Maharashtra is a very large state of 300,000 km2, with a total population of around 97 million. The capital city of Maharashtra, Mumbai, is the most populous city in India, with around 14 million inhabitants. The HIV prevalence at antenatal clinics in Maharashtra was 0.5% in 2007. The state has the highest reported rates of HIV prevalence among female sex workers (18%). Similarly high rates were found among injecting drug users (24%) and homosexual men (12%). Pune is the second largest city in Maharashtra, with a growing population of more than 40 lakhs (4 million). It ranks among the top five HIV prevalent cities in the state. There are very few studies that have been carried out to compare the prevalence of intestinal parasitic infestation in HIV-reactive and non-reactive individuals in Maharashtra. Materials and Methods- Study Period- The present study was carried out from 1st December 2008 to 31st August 2010 in Pad. Dr. D.Y. Patil Medical College Hospital and Research Center, Pimpri, Pune. Results and Observations- In this study, stool samples of 490 individuals were processed, out of which 110 were HIV-positive and 380 were HIV-negative. Evaluation of 4 different stool concentration techniques was done in comparison with the direct wet mount microscopic examination. Out of all the stool samples examined, 100 of them were also processed using concentration techniques (by all methods). It was seen that using routine examination, only 6% of the stool samples revealed a positive finding, whereas using concentration techniques a maximum of 17% of the same samples were positive. Conclusion- Further, as demonstrated in our study, we can conclude that stool concentration techniques should be adopted, since in case of low parasite load, often the diagnosis is missed by carrying out only direct wet mount examination. Finally, to prevent intestinal parasitic infections, patients should be educated regarding maintenance of personal hygiene.
intestinal parasites, Ascaris lumbricoides, H. nana, T. solium, T. saginata.
India is one of the largest and most populated countries in the world, with over one billion inhabitants. Of this number, it's estimated that around 2.3 million people are currently living with the human immunodeficiency virus (HIV) [1,2] . Maharashtra is a very large state of 300,000 km2, with a total population of around 97 million. The capital city of Maharashtra, Mumbai, is the most populous city in India, with around 14 million inhabitants. The HIV prevalence at antenatal clinics in Maharashtra was 0.5% in 2007. The state has the highest reported rates of HIV prevalence among female sex workers (18%). Similarly high rates were found among injecting drug users (24%) and homosexual men (12%). Pune is the second largest city in Maharashtra, with a growing population of more than 40 lakhs (4 million) [3,4-6] . It ranks among the top five HIV prevalent cities in the state. Official figures report that in Jan-Oct 2007, 18,039 people in the city were tested for HIV at government testing centres. Of these, 12.27% tested positive. These figures exclude the thousands of people already living with HIV in Pune, along with those who are as yet unaware of their HIV positive status. Several species of protozoa have been associated with acute and chronic diarrhea in HIV disease [7-9] . The most commonly reported include Cryptosporidium parvum, lsospora belli, Microsporidium species, Giardia intestinalis, Entamoeba histolytica and Cyclospora species. Besides these, the nematode Strongyloides stercoralis can cause diarrhea and overwhelming infestation (hyperinfection syndrome) in patients with such immunosuppressive disorders [7-9,10-14] .
Intestinal parasitic infestations represent a large and serious medical and public health problem in developing countries. Intestinal parasitosis is a major health problem in India. Slum dwellers have high rates of infestation due to poor sanitation, contaminated water supply and high population density. Their nutritional status could also be an important factor, as most of them are chronically undernourished. Infection and malnutrition have a synergistic association. There are very few studies that have been carried out to compare the prevalence of intestinal parasitic infestation in HIV-reactive and non-reactive individuals in Maharashtra. The patients attending our hospital are generally very poor. The principle inhabitants of the nearby area are poor unskilled workers and also migrants from rural areas. They often do not have access to potable water and live under unhygienic conditions. Over-crowding and improper sewage are also common in this area [13-18] . As a result, intestinal parasitic infestations are often encountered. Further, many of these people are HIV positive due to lack of knowledge regarding the disease and how it is transmitted. Often these people presented to the hospital with signs and symptoms of opportunistic infections like diarrhea due to intestinal parasites and were incidentally detected to be HIV positive in the course of treatment. Keeping this in mind, the present study was undertaken in D.Y. Patil Medical College Hospital and Research Center, Pimpri, Pune-18 India.
Study Period- The present study was carried out from 1st December 2008 to 31st August 2010 in Pd. Dr. D.Y. Patil Medical College Hospital and Research Center, Pimpri, Pune. Study Group-Data obtained from all patients included information regarding name, age and sex of the patient, as well as symptoms and duration of illness.
Ethics Statement- Written informed consents were obtained from all patients and study protocol were approved by the institutional ethics committee of Dr. D. Y. Patil Medical College, Pune.
Sample Collection- Stool samples were collected from OPD and IPD patients with or without abdominal symptoms, at the time of presentation to the hospital. Patients positive for HIV by ‘TRI-DOT’, followed by confirmation, as per available record from Central Clinical Laboratory (CCL). All stool samples, for parasitological investigations, were processed in the Department of Microbiology, Pd. Dr. D.Y. Patil Medical College Hospital and Research Center, Pimpri, Pune.
‘TRI-DOT’ Test- The HIV ‘TRI-DOT’ test is a visual, rapid, sensitive and accurate immunoassay for the differential detection of HIV-1 and HIV-2 antibodies (IgG) in the human serum or plasma using HIV-1 and HIV-2 antigens immobilized in an immunofiltration membrane. The test is a screening test for anti-HIV-1 and anti-HIV-2 and is for in vitro diagnostic use only [10-21] .
Interpretation of Results- Non-reactive: If only one dot (the control dot) appears, the specimen is non-reactive for antibodies to either to HIV-1 or HIV-2. Reactive: If two dots, one for the control and the other for HIV-1 appear, the specimen is reactive for antibodies to HIV-1. If two dots, one for the control and the other for HIV-2 appear, the specimen is reactive for antibodies to HIV-2. If all the three dots, one each for control, HIV-1 and HIV-2 appear, the specimen is reactive for antibodies to both HIV-1 and HIV-2.
Collection of Stool-The following essentials were fulfilled:
• Sterile universal container was used or a clean and dry container
• Patient was instructed not to mix urine with stool sample
Oil, oily emulsion, barium or bismuth salts were not given to the patients before stool examination [22-26] .
Wet mount-The identification of intestinal parasites was done by using a good binocular microscope under 10x and confirmed by observing under 40x [22-28,29-33] .
A portion of the stool is picked up using a wooden stick or a nichrome loop and mixed with a drop of normal saline (0.9%) on a glass slide. The preparation was covered with a cover slip and observed under the microscope-Iodine Preparation - A portion of stool was picked up using a wooden stick or a nichrome loop and mixed with a drop of dilute Lugol’s iodine on the other end of the same slide on which the saline preparation was done. It was covered with a coverslip and observed under the microscope.
Permanent Stain- The detection and correct identification of intestinal protozoa frequently depend on the examination of the permanent stained smear.
Procedure- The smear is covered with a rectangular piece of filter paper and 5-7 drops of carbol fuschin is applied to thoroughly moisten the filter paper for 5 min. No heating is required. The paper is removed with a pair of forceps and the slide rinsed with water. The smear is decolorized with acid-alcohol, till no more stain appears in the washing. Then, it is counterstained with methlene blue for 1-2 min. Finally, the smear is rinsed, drained, air dried and examined under oil immersion (100x) [25-30] .
Procedure- The smear was fixed with methyl alcohol. Mixture of one part of stain and ten parts of buffer solution was applied for 1 h. The smear was washed with buffer solution, allowing preparation to differentiate for about 30 sec. The slide was blot dried and observed under oil immersion (100x).
Various means of concentration of intestinal parasites have been devised so that they can be easily found. The procedure carried out for the concentration of parasites is carried out by sedimentation or floatation.
Floatation Techniques- Simple floatation technique-Procedure: 1ml of faeces was taken in the container and few drops of salt solution were added. It was then stirred with a glass rod so as to make an even emulsion. After this, more salt solution was added till the container was nearly full. Coarse matter, which floated up, was removed. The container was placed on a level surface and the final filling of the glass container was done with the help of a dropper until, a convex meniscus was formed. A glass slide was carefully laid on top of the container so that its center was in contact with the fluid. The preparation was allowed to stand for 20-30 min after which the glass slide was quickly lifted, turned over smoothly so as to prevent spillage of the liquid and examined under the microscope. A coverslip was not placed on top of the fluid.
Procedure- A fine faecal suspension was made by taking 1g of freshly passed stool and 10ml of lukewarm distilled water. The coarse particles were removed by straining through a wire gauge. The filtrate was collected in a tube and centrifuged for 1 min at the rate of 2500 revolutions per min (rpm). The supernatant fluid was poured off and distilled water was added to the sediment. It was shaken well, centrifuged and the procedure was repeated two to three times till the supernatant fluid became clear, which was then poured off. To the sediment was added 3-4 ml of a 33% zinc sulphate solution having a specific gravity of 1.8. The sediment was stirred and further zinc sulphate solution was added to fill the tube up to the top and centrifuged again for at least 1 min at 2500 rpm. The surface film was then removed by a nichrome loop on to a glass slide, covered by a cover slip and observed under the microscope.
Procedure- A sufficient amount of faeces was taken and thoroughly shaken with about twenty times its volume of tap water. It was allowed to settle in a conical flask for two hours. The process was repeated several times till the supernatant fluid was clear. Finally, the sediment at the bottom was examined for the eggs. This process was not suitable for protozoal cysts.
Procedure- 1g of farces was emulsified in 7ml of 10% formal-saline and kept for 10min, for fixation. It was then strained through a wire gauge and the filtrate was collected in a centrifuge tube. 3ml of ether was added to it and the mixture was shaken vigorously for 1min. It was then centrifuged at 2,000 rpm for 2min and then allowed to settle. The debris was loosened with a stick, the upper part of the test tube was cleared of fatty debris and the supernatant fluid was decanted, leaving 1 or 2 drops. The deposit, after shaking, was poured on to a glass slide, a cover slip placed over it and the specimen was examined. This process was suitable for both protozoal cysts and helminthes eggs [29-34] .
In this study, stool samples of 490 individuals were processed, out of which 110 were HIV-positive and 380 were HIV-negative.
Stool samples of 110 HIV-positive individuals were processed. HIV status was determined by carrying out the ‘TRI-DOT’ test, followed by confirmation. Of the 110 patients, 19(17.2%) had diarrhea as a symptom, whereas 91(82.8%) did not. Intestinal parasites were isolated in 33 of them (30%) showed in [Table-1] .
Out of the 19 patients with diarrhea, 16(84.2%) had stool examination positive for parasites; whereas of the remaining 91 without diarrhea only 17(18.7%) had intestinal parasites detected in their stool samples. This is depicted in [Table-2] and [Fig-1] HIV-positive patients, the prevalence of intestinal parasites in patients with diarrhea was significantly more than in those without diarrhea (P < 0.0001).
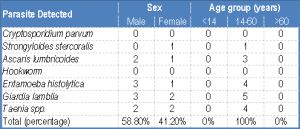
The difference in the prevalence between males and females, however, was not statistically significant (P > 0.05) [Table-3] .
HIV-Negative patients, as mentioned in [Table-1] , stool samples of 380 HIV-negative individuals were also examined. Amongst them, 220(58%) had abdominal symptoms like altered bowel habit and abdominal pain, whereas 160(42%) were asymptomatic. Intestinal parasites were detected in 55(14.4%) of the 380 patients. Prevalence of intestinal parasites in HIV-negative patients - Amongst the 220 symptomatic patients, intestinal parasites were detected in 38(17.3%), whereas only 17(10.6%) amongst the 160 asymptomatic patients had intestinal parasites. This is depicted in [Table-5] and Fig-3 .
In this study, Formol-ether sedimentation technique and Zinc-sulphate floatation technique were found to be better in isolating all types of intestinal parasites, compared to the other methods. Saturated-salt solution floatation technique was found to be particularly effective in the concentration of Ascaris and simple sedimentation was found particularly effective in the concentration of eggs of Taenia spp.
HIV infection, a worldwide infection, is a serious problem in the present day. One of the major health problems among HIV seropositive patients in the presence of opportunistic infection. Furthermore, intestinal parasitic infection, which is also one of the basic health problems in tropical regions, is common in these patients. In the present study, stool samples of 110 HIV-positive individuals and 380 HIV-negative were processed. Intestinal parasites were isolated in 33(30%) and 55(14.4%) from HIV-positive and HIV-negative respectively. It was found that prevalence of intestinal parasites is more in HIV-positive individuals compared to HIV-negative individuals. Gupta, et al. also saw similar results in a study where they found that prevalence of intestinal parasites was higher in HIV-positive individuals (28.3%) compared to HIV-negative individuals (11.5%). A similar comparative study to ours was carried out in Wardha, Maharashtra where it was found that the total number of intestinal parasites observed in the stool samples of HIV seropositive patients was 87(58.8%) as compared to 36(30%) in the stool samples of HIV seronegative patients [5-10] . Similar results have also been reported from various other studies in India. Observations of Brink, et al. in a study in Uganda, Africa, Weber, et al. in a study in Switzerland and Gomez, et al. in a study in Tanzania, Africa are in agreement with our results [18-22] .
Out of the 110 HIV-positive patients, only 19(17.2%) had diarrhea as a symptom. Of these patients, 16(84.2%) had stool examination positive for parasites. The etiologic spectrum of enteric pathogens causing diarrhea in HIV includes bacteria, parasites, fungi and viruses. This may explain the absence of any intestinal parasite in the remaining 3 patients with diarrhea. Of the remaining 91 patients without diarrhea, only 17(18.7%) had intestinal parasites detected in their stool. Majority of the patients, seen at our hospital, were already on HAART or other symptomatic treatment prior to their visit and therefore the number of symptomatic patients were less. Many of the patients were also recently infected cases and therefore were not significantly immunocompromised. Further, amongst the HIV-positive patients with diarrhea, oocysts of Cryptosporidium parvum and motile trophozoites of Entamoeba histolytica were present in the stool samples of 4 patients (25%), motile rhabditiform larva of Strongyloides stercoralis and motile trophozoites of Giardia lamblia in 3(18.8%) and in 2 other patients, egg of hookworm were detected (12.5%). Therefore, in this study, the most common parasites to be isolated in HIV-positive patients with diarrhea were oocysts of Cryptosporidium and trophozoites of Entamoeba histolytica. Cryptosporidium parvum was found to be the most commonly isolated parasite in HIV-positive patients with diarrhea in a study carried out by Kulkarni, et al. However, in their study, Entamoeba spp was the third most commonly isolated intestinal parasite. Cryptosporidium was also the leading parasite to be detected in a study carried out by Mohandas, et al [18-22,28-33] .
It was also seen that prevalence of intestinal parasites was significantly higher in HIV-patients with diarrhea compared to those without diarrhea [Table-2] . This observation is in agreement to the study by Kumar S.S., et al. as well as Wiwanitkit. We found that apart from the opportunistic intestinal parasites like Cryptosporidium, non-opportunistic infections, like Taenia and Ascaris, were also common in HIV-positive patients. Interestingly, most of the HIV-positive patients who were included in this study were males in the 14-60 years age group [Table-4] , [Fig-2] . Predominance of male cases may be due to their migration to the metropolitan cities in search of work. Staying away from the families for longer periods and males being promiscuous by habit resulted in them acquiring HIV infection. However, there was no statistically significant difference in the prevalence of intestinal parasites between males and females. This is probably due to the fact that most of the subjects in this study were inhabitants of the same region and were exposed to similar risk factors for acquiring intestinal parasitic infection viz. common water supply, similar food habits, overcrowding [29-34] .
Prevalence of intestinal parasites in HIV-negative patients- Stool samples of 380 HIV-negative individuals were also screened for parasites. 220(58%) of them had some abdominal symptoms, like altered bowel habits, abdominal pain etc. while 160(42%) were asymptomatic. It was seen that 38(17.3%) of the patients with abdominal symptoms had intestinal parasites in their stool. On the other hand 17(10.6%) of the patients who had no significant abdominal symptoms had parasites in their intestine. This difference was not statistically significant. From this observation we can conclude that intestinal parasitic infection does not always give rise to significant abdominal symptoms and therefore stool examination should be carried out meticulously as a routine in all patients attending the hospital. Taenia spp. was the most commonly encountered intestinal parasite in both the symptomatic and asymptomatic group. The reason behind this could be that the majority of people attending our hospital belong to the lower socio-economic strata, living in nearby areas where consumption of pork and beef are very common. Also, pigs and cows are commonly seen to graze in the fields where vegetables are grown. Thereby, consumption of improperly cooked vegetables and salads also puts the vegetarians at risk. In addition, these areas have poor sanitation facilities and most of the people are unaware about general hygiene. In a study carried out by Nagaraj, et al. they found Ascaris to be the most commonly isolated parasite and hookworm to be less common. In our study also hookworm isolation was less compared to the others. The prevalence of hookworm is usually low in urban slums as agricultural activity is required to maintain high levels of its transmission. Moreover, most of the subjects use footwear regularly, thus minimizing the chance for contact.
Amongst the nematodes, the most common parasite isolated was Ascaris followed by hookworm and then Trichuris, which is in agreement to the study carried out by Gadgil, et al. [22-28] . Enterobius was not detected in this study probably because NIH swab technique was not adopted.
Further, it was seen that intestinal parasites were more common in male patients between the 14-60 yrs. age group. This is the group who work outside and do not always have access to home-cooked food and potable water. In a study in Nepal, it was found that intestinal parasites were more common amongst women. On the contrary, Sethi, et al. [32-40] , in a study in Chandigarh, found men are more prone to get infected by intestinal parasites compared to women. Therefore, we can infer that variation in the prevalence of intestinal parasites amongst the sexes is unique to the place where the study is carried. Intestinal parasites were also seen in children, especially the school going age group. This can be explained by the fact that children often come in contact with contaminated soil while playing in parks and often consume food and water without proper hand-washing.
Intestinal parasitic infections are highly prevalent in the Pimpri-Chinchwad area, amongst both HIV-positive and HIV-negative individuals. However, the prevalence of intestinal parasites in the HIV-positive group was significantly more compared to the HIV-negative patients. Apart from the opportunistic infections, which are common in immunocompromised patients, tropical endemic non-opportunistic intestinal parasites also infect these patients. In contrast, opportunistic parasites were not detected in HIV-negative patients. Therefore, this study emphasizes the importance of meticulous stool examination, which can act as a competent tool to guide the clinicians in the treatment of their patients. Further, as demonstrated in our study, we can conclude that stool concentration techniques should be adopted, since in case of low parasite load, often the diagnosis is missed by carrying out only direct wet mount examination. Finally, to prevent intestinal parasitic infections, patients should be educated regarding maintenance of personal hygiene.
[1] National Aids Control Organization (2007) A Technical Brief., 1-24.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
[2] Ghosh T.K. (1986) J. Indian Med. Assoc., 84(1), 29-30.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
[3] UNAIDS (2010) India-country Progress Report.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
[4] Tuli L., Gulati A.K., Sundar S., Mohapatra T.M. (2008) BMC Gastroenterol., 8-36.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
[5] Gupta S., Narang S., Nunavath V., Singh S. (2008) Indian J. Med. Microbiol., 26, 172-5.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
[6] Hegde G.R., Patel J.C. (1986) J. Postgrad. Med., 32(4), 225-8.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
[7] Nagaraj S., Raghavan R., Macaden R., Kurpad A.V. (2004) Indian J. Med. Microbiol., 22(1), 54-6.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
[8] CoCCOCox FEG (2002) Clin. Microbiol. Rev., 15(4), 595-612.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
[9] Jimenez J.A., Rodriguez S., Moyano L.M., Castillo Y., Garcia H.H. (2010) Trop. Med. Int. Health., 15(9), 1077-81.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
[10] Del Brutto O.H., Santibanez R., Noboa C.A., Aguirre R., Diaz E., Alarcon T.A. (1992) Neurology, 42, 389-92.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
[11] Fan P.C., Lin C.Y., Chen C.C., Chung W.C. (1995) J. Helminthol., 69(4), 299-303.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
[12] Wasadikar P.P., Kulkami A.B. (1997) Br. J. Surg., 84, 410-2.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
[13] Grove D.I. (1996) Adv. Parasitol., 38, 251-309.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
[14] Scowden E.B., Schaffner W., Stone W.J. (1978) Medicine, 57, 527-44.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
[15] Adedayo O., Grell G., Bellot P. (2002) South Med. J., 95, 711-6.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
[16] Siddiqui A.A., Berk S.L. (2001) Clin. Infect. Dis., 33, 1040-7.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
[17] Loutfy M.R., Wilson M., Keystone J.S., Kain K.C. (2002) Am. J. Trop. Med. Hyg., 66(6), 749-52.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
[18] WHO Expert Committee (2002) Tech. Rep. Ser., 912, 1-53.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
[19] Roche M., Layrisse M. (1966) Am. J. Trop. Med. Hyg., 15(6), 1032-102.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
[20] Migasena S., Gilles H.M. (1987) Clin. Trop. Med. Comm. Dis., 2, 617-27.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
[21] Gilles H.M., Williams E.J.W., Ball P.A.J. (1964) Q. J. Med., 33, 1-24.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
[22] Maxwell C., Hussain R., Nutman T.B., et al. (1987) Am. J. Trop. Med. Hyg., 37(1), 126-34.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
[23] Diemert D.J., Bethony J.M., Hotez P.J. (2008) J. Clin. Infect. Dis., 282-8.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
[24] Gandhi D., Srivastava D.N., Batra B., Chandra S. (1999) Indian Pediatr., 36, 1270-2.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
[25] Crompton DWT (2001) Adv. Parasitol., 48, 285-375.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
[26] DeSilva N.R., Chan M.S., Bundy D.A. (1997) Trop. Med. Int. Health., 2, 519-28.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
[27] Albonico M., Crompton D.W., Savioli L. (1999) Adv. Parasitol., 42, 277-341.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
[28] O’Lorcain P., Holland C.V. (2000) Suppl., S1, S51-71.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
[29] Wakelin D., Farias S.E., Bradley J.E. (2002) Parasitology, 125(7), S39-50.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
[30] Williams-Blangero S., VandeBerg J.L., Subedi J., Aivaliotis M.J., Rai D.R., Upadhayay R.P., et al. (2002) Proc. Natl. Acad. Sci. USA, 99, 5533-8.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
[31] Quinell R.J. (2003) Int. J. Parasitol., 33, 1219-31.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
[32] Gelpi A.P., Mustafa A. (1968) Am. J. Med., 44, 377-89.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
[33] Strephenson LS.(1980) Parasitology;81:221-33.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
[34] Crompton DW, Nesheim MC. (2002) Annu Rev Nutr;22:35-59.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
[35] Willett W.C., Kilama W.L., Kihamia C.M. (1979) Am. J. Public Health, 69, 987-91.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
[36] Archibong A.E., Ndoma-Egba R., Asindi A.A. (1994) East Afr. Med. J., 71, 286-9.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
[37] Blumenthal D.S., Schultz M.G. (1975) Am. J. Trop. Med. Hyg., 24, 801-805.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
[38] De Silva N.R., Chan M.S., Bundy D.A. (1997) Trop. Med. Hyg., 91, 31-6.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
[39] Khuroo M.S., Zargar S.A., Mahajan R. (1990) Lancet., 335, 1503-8.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
[40] Valgaeren G., Duysburgh I., Fierens H., et al. (1996) Acta. Clin. Belg., 51, 97-100.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
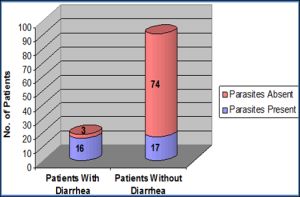 | Fig. 1- Prevalence of parasites in HIV-positive patients. |
 | Fig. 2- Comparison of the common intestinal parasites detected |
 | Table 1- Total number of samples processed |
 | Table 2- Prevalence of intestinal parasites in HIV-positive patients |
 | Table 3- Sex-wise prevalence of intestinal parasites in HIV-positive patients with diarrhea |
 | Table 4- Intestinal parasites detected in HIV-positive patients without diarrhea and their correlation with age and sex |
 | Table 5- Prevalence of parasitic infestations by different concentration methods in comparison to direct wet mount examination |