ISSN : 0975-2862
EISSN : 0975-9158
AJIT KUMAR SAXENA1*
1Human Cytogenetics & Molecular Genetic Laboratory, Faculty of Medicine, Centre of Experimental Medicine & Surgery and Institute of Medical Sciences, Banaras Hindu University, Varanasi-221005, India
* Corresponding Author : draksaxena1@rediffmail.com
Received : 17-08-2011 Accepted : 24-09-2011 Published : 15-12-2011
Volume : 3 Issue : 2 Pages : 47 - 49
Genetics 3.2 (2011):47-49
DOI : http://dx.doi.org/10.9735/0975-2862.3.2.47-49
Conflict of Interest : None declared
MTHFR gene polymorphism regulate folate metabolism, required for normal development of central nervous system and any error in metabolism either due to hereditary or sporadic gene mutation in the family lead to the development of mental retardation in heterozygous condition. In the present study the five families having severe congenital mental retardation was evaluated for C677T genotype variations i.e. CC, CT & TT in probands, mother & father using PCR-RFLP analysis. Highest frequency (60%) was observed in heterozygous condition in the mother of proband. Statistical analysis showing significant difference (p=0.024) were observed in the father of the proband. Interestingly, the insertion of 68bp of CβS gene mutation was also observed in father of one family suggesting paternal or maternal factors influencing for severe mental retardation in children of consanguineous families as an independent risk factor. However, the high degree of genetic heterogeneity is quite striking because of severe mutation in two families. The pedigree analysis showing that the severity of disease transmission probably due to the penetrance of gene and their mode of inheritance is autosomal recessive in nature.
Gene polymorphism, mental retardation, PCR, RFLP analysis, Consanguineous.
MTHFR gene increased risk for mental retardation.
Globally, mental retardation have high prevalence in the world (2.3%) and 1 to 3% population of developed countries are suffer from a common cognitive impairment of mental retardation [1,2] . Large number of environmental and genetic factor is responsible for mental retardation including premature birth, prenatal infections, chromosomal abnormalities and single-gene mutations [3] . Because of variable penetrance of gene are accountable for phenotypic expression in hereditary syndromes. There are challenges of understanding the biological basis of hereditary due to genetic heterogeneity and limited knowledge. Large numbers of genes are listed in Mendelian inheritance in databases and bioinformatics: OMIM database - Institute for Genetic Medicine, Johns Hopkins University and National Center for Biotechnology [4] . In human 282 mutated genes are responsible for mental retardation and few are located on X-chromosome [5] . Interestingly, severe mental retardation is one of the major characteristics of imprinting disorders in genes normally expressed monoallelically from either the maternal or paternal copy depending on its epigenetic state.
Gene polymorphism C677T has been associated with mental retardation and other complex congenital anomalies [6] . MTHFR variants codes thermolabile enzyme has been linked to increase homocysteine level in C677T individuals having deficiency of folate [7] . Because MTHFR involvement and intelligence quotient in down syndromes has been associated with “risk factor†in infants in homozygous C677T genotype for severe mental retardation [8] . Although, the role of MTHFR C677T gene polymorphism is not yet properly understood but it is believed that either paternal or maternal factor contribute the etiologies of congenital “birth defects†leads to the mental retardation between consaguineous and nonconsanguineous parents with variable phenotypic effects. MTHFR catalyses irreversibly conversion of 5,10-methylenetetrahydrofolate to 5-methyltetrahydrofolate, which is the methyl donor for methionine synthesis from homocysteine and participates in S-adenosyl methionine synthesis and DNA methylation. Folate is an essential component for the development of central nervous system during organogenesis and any error leads to abnormal differentiation cause mental retardation [9] . Folic acid deficiency leads to increase plasma homocysteine C677T in an individual’s known to increase genetic risk factor and chromosomal instability for various clinical lesion including NTDs [10,11,12,13] . Although, the role of MTHFR gene polymorphism is not yet properly understood but it is believed that either paternal or maternal factor alone or both contribute the etiologies of congenital “birth defects†leads to the severe mental retardation in children between consanguineous and nonconsanguineous families with variable phenotypes.
Here we are presenting the interesting cases (probands) of mental retardation with data of five families including both consanguineous & non – consanguineous families as shown in [Fig-2ab] . The age group of proband varies between 4-10 years with variable karyotypic findings including normal 46, XY; Trisomy-21; FRAX, Mosaic (46/47, XX). Deliveries were normal with full term. The mean age 33.5 years of mother of proband with cytogenetic finding shows normal karyotypic feature while father of the proband shows out of five two were mosaic (46,XX/47, XX karyotype) and father mean age 27 years with normal phenotypes. Blood samples (1.0 ml) were collected in EDTA for isolation of genomic DNA using standard laboratory procedure. MTHFR Primers C677T (F-5'TGAAGGAGAAGGTGTCTGCGGGA3') & (R- 5'AGGACGGTGCGGTGAGAGTG3') Restriction fragment length polymorphism (RFLP) analysis was carried out to determined missence mutation in the presence of HinfI as reported by Frosst et al (1995). PCR product (6 µl) were digested at 37ºC for 3hr. in reaction volume of 25 µl containing 1U of Hinf-I restriction enzyme (New England, Biolabs) and NEB buffer (2.5 µl). Digested product of RFLP was separated on 3% agarose gel stained with EtBr and visualized on Gel Doc system (SR Biosystem). CβS gene mutation, DNA was amplified using specific primers to amplify the 844 ins68 polymorphism in the exon 8 and flanking intron 7 forward 5’-GTTGTTAACGGCGGTATTGC-3’ and reveres 5’-GTTGTCTGCTCCGTCTGGTT-3’. PCR was carried out by using specific forward and reverse primers in total volume of 25 µl contain 50-100 ng of genomic DNA, 20 pmole of each primer, 200µM of each dNTPs mix with Taq buffer (10mM Tris HCl pH 8.3, 50mM KCl), 3.0mM MgCl2 and 3 unit of Taq polymerase (New England Biolab). Cycling conditions were 4 min at 94ºC for initial denaturation, 58 ºC/1min for annealing followed by 35 cycles and 72 ºC/7min for final extension. The analysis was performed with the PCR product was separated and visualized on 1.5 % agarose & documented in a Gel DocTM EQ (SR Biosystem).
In heterozygous (CT) condition the highest frequency (60%) was observed in mothers when compared with proband (25%), although, the elevated frequency (75%) of homozygous CC genotype was also seen in probands. The changes in the variation of frequency between homozygous and heterozygous are either due to non random mating and uneven gene flow or unknown biological relevance. The elevated frequency of CT genotype may increase risk for development of mentally retarded children. However, statistical analysis shows lack of significant (p< 0.05) difference using chi- square test, but significant differences were observed (p=0.024) in father of the probands suggesting that paternal factor might have influencing factor for severe mental retardation as an independent risk factor. Out of five families two mothers of the proband are in heterozygous state (CT) while father showing the complete disappearance of 198 bp amplicon of MTHFR C677T gene. Interestingly, the father of the one proband showing insertion of 68bp in CβS gene mutation in nonconsanguineous family [Fig-1b] .
This is the first case report showing involvement of either maternal or paternal or both factors increase risk for severe mental retardation has not been documented earlier in this region. The pedigree analysis indicates that folate related mechanism are important to evaluate the mode of transmission of illness in cases of consanguineous families because maternal / paternal (hereditary) factor involving double copy of MTHFR gene mutation responsible to increase severe risk for clinical lesion such as mental retardation. Numerous studies has been showing neurological disorder associated with MTHFR C677T polymorphisms and the intelligence quotient in patients with trisomy-21 including risk for complex congenital anomalies [14,15,9] . However, there is lack of correlation exist between karyotypic variation and molecular analysis in probands & their parents. In the present study the identification of MTHFR mutation in such families add another level of complexity between genotype and phenotype. We hypothesized that infants with homozygous (TT) or heterozygous (CT) state of C677T genotype would be at “ higher risk†for severe mental retardation although, the mode of inheritance from mother to the son / daughter is complicated but alleles segregation might have responsible for severity of the disease. Such mutation exists either in heterozygous or homozygous state may correlated with reduced enzyme activity and significantly increased plasma homocysteine with folate deficiency at higher risk of neurodegenerative disorders as an independent risk factor in arterial disease and neural tube defects [15,16,12] . The severity of disease in proband is either due to the penetrance of gene or segregation of allele as shown in the pedigree analysis showing the mode of inheritance autosomal recessive in nature.
In this present study we concluded that there are four possible reasons associated with severity of disease in proband –
1. MTHFR polymorphism in heterozygous (CT) condition increased risk as an independent factor for mental retardation, 2. Maternal age is also equally important for developing complications during foetal life, 3. Paternal factor include CβS gene mutation which confirm to alters homocysteine metabolism, and (4) Increased risk in consanguineous families probably due to extra copy of allele (mutated) implicated high risk factor of severe mental retardation.
Author AKS is thankful to the families of the proband for such study who referred from S S Hospital of IMS to Human Cytogenetic laboratory, CEMS, IMS for genomic analysis.
There is no conflict of interest between the authors and family members.
[1] Roeleveld N., Zielhuis G. A. and Gabreels F. (1997) Dev. Med. Child Neurol, 39, 125–132.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
[2] Aicardi J. (1998) Semin. Pediatr. Neurol., 5: 15–20.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
[3] Kinsbourne M. and Graf W. D. (2000) Disorders of mental development,. in Child Neurology, edited by J. H. Menkes and H. B. Sarnat. Lippincott Williams & Wilkins, Philadelphia, 1155–1211.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
[4] Hamosh A., Scott A. F., Amberger J., Bocchini C., Valle D. et al., (2002) Nucleic Acids Res., 30, 255–382.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
[5] Jensen L. R., Chen W., Moser B., Lipkowitz B., Schroeder C., Musante L., et al. (2011) Eur J Hum Genet. 244.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
[6] Botto L.D., Yang Q. (2000) Am J Epidemiol, 151, 862-877.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
[7] Frosst P., Blom H.J., Milos R., Goyette P., Sheppard C.A., Matthews R.G., Boers G.J.H., et al (1995) Nat Genet, 10, 111-113.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
[8] Shaw G. M., Jelliffe-Pawlowski L., Nelson V., Zhu H., Harris J. A. & Finnell R. H. (2007) Birth Defects Res.79, 24–26.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
[9] Gueant J.L., Anello G., Bosco P., et al. (2005) J Neurol Neurosurg Psychiatry, 76, 706–709.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
[10] Boushey C., Beresford S.A.A., Omenn G.S., Motulsky A.G. (1995) JAMA, 274, 1049-1057.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
[11] Kluijtmans L.A.J., Boers G.H.J., Trijbels F.J.M., Van Lith-Zanders H.M.A., van den Heuvel L.P.W.J., Blom H.J.M. (1997) Biochem and Mol Med, 62, 23-25.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
[12] Ajit K Saxena, Jyoti Gupta, Divya Singh, (2011 (in press).
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
[13] James S.J., Pogribna M., Pogribny I.P., et al. (1999) Am J Clin Nutr; 70, 495–501.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
[14] Hobbs C.A., Sherman S.L., Yi P., et al.(2000) Am J Hum Genet, 67, 623–630.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
[15] Nilsson K., Gustafson L., Hultberg B. (2000) Clin Chem, 46, 691–6.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
[16] Orendac M., Muskova B., Richterova F., Zvarova J., Stefek M., Zaykova E., Stribrny J.,Hyanek J., Kraus J.P., Kozich V. (1998) Neth J Med, 47-52.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
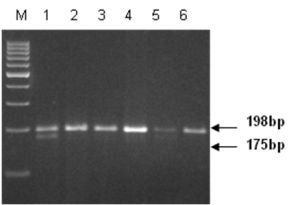 | Fig. 1a- MTHFR C677T gene polymorphism in mental retarded cases (proband) and their parents. Lane 1 mother, lane 2, 4 & 6 father, lane 3 & 5 proband. Lane 1 & 5 showing CT genotype while 2, 3,4,5 & 6 are CC genotype, Lane-M 100bp ladder |
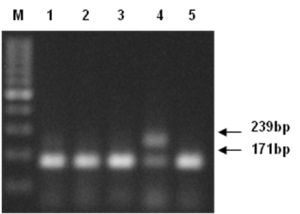 | Fig. 1b- CβS gene analysis. Lane- 1 & 3 mother; Lane 2 & 4 father, Lane 5 proband. Lane 4 showing insertion of 68bp of CβS gene in father of mental retarded case. M 100bp ladder |
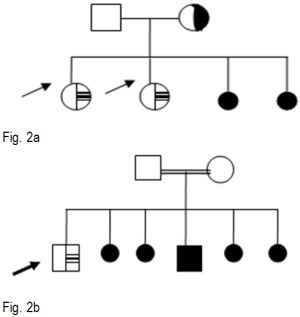 | Fig. 2(a,b)- Representative pedigree analysis showing the severity in probands between consanguineous (B) and nonconsanguineous (A) families. Mother of the proband showing CT genotype of MTHFR C677T (fig.2A) while father showing the complete disappearance of 198bp amplicon of C677T (figure. 2B). The severity in the probands due to the penetrance of gene (s) in autosomal recessive condition. |