ISSN : 0976-5530
EISSN : 0976-5549

KUMUD HARLEY1*, SANJAY PRAMANIK2, ANJALI VAGGA3
1Department of Biochemistry, JNMC (DMIMSU) Sawangi (M), Wardha
2Department of Biochemistry, GMC-SSH, Nagpur
3Department of Biochemistry, JNMC (DMIMSU) Sawangi (M), Wardha
* Corresponding Author : drkharley@gmail.com, hkumud@yahoo.com
Received : 29-10-2011 Accepted : 30-11-2011 Published : 27-12-2011
Volume : 2 Issue : 2 Pages : 98 - 100
Int J Med Clin Res 2.2 (2011):98-100
DOI : http://dx.doi.org/10.9735/0976-5530.2.2.98-100
Conflict of Interest : None declared
Selenium is a trace element that plays role in antioxidant defense mechanism via selenium dependent glutathione peroxidases (GSH-PX) and selenoproteins. When selenium is lacking, the intima of the arteries is prone to get oxidative damage and involve in development of atherosclerosis. It has been observed in clinical studies that the serum selenium levels in patients with myocardial infarction and with angina pectoris have been significantly lower than that in healthy people. In the present study we found significantly low concentration of serum selenium in acute myocardial infarction (AMI) compared with the age and sex matched healthy controls with p value less than 0.001.
Selenium, Glutathione Peroxidase (GSH-PX), Acute Myocardial infarction (AMI), antioxidant.
Coronary artery disease (CAD) is disease which has serious impacts on human health and safety. There are many reasons that induce atherosclerosis. One of the reasons is that selenium is a strong antioxidant. In addition, the selenium participates in stabilization and repair of damaged myocardial cell membranes and repair of damaged myocardial cell membranes as well as in the maintenance of normal function of cells. When lacking selenium, peroxidation of the coronary artery (intimal layer) increases and thus the risk for coronary artery disease development [1,2] . Evidence shows that oxygen derived free radicals are important mediators of oxidation of lipoproteins leading to endothelial damage and are said to play a role in myocardial tissue damage [3] .
With growing interest in the concept of free radicals and role of selenium. The current study was designed with aim to assess the role of serum selenium and glutathione peroxidase in preventing the risk of development of atherosclerosis and thus in preventing acute myocardial infarction.
Case- control study was conducted on 36 patients of acute myocardial infarction admitted in the ICCU in Department of Medicine at Government Medical College, Nagpur. 36 matched healthy individuals were selected as controls for the study. AMI patients were diagnosed on the basis of WHO criteria of clinical history suggestive of myocardial infarction i.e. ECG-findings suggestive of myocardial infarction (MI), and elevation of biochemical markers (creatinine kinase, and CK-MB). All were assessed for risk factors like Diabetes mellitus, hypertension, obesity, smoking and a parental history of ischemic heart disease (IHD). Age and sex matched apparently healthy controls were also selected having no history of chest pain, vomiting, sweating and ECG- findings not suggesting of signs of myocardial infarction and CK-MB levels within normal limits.
10 ml sample was drawn from anticubital vein of the patients within 6 hours from the complaints of chest pain and controls with informed oral consent and following biochemical parameters were evaluated
*Serum triglycerides by Dynamic extended stability (DES) [4] with lipid lowering agents, GPO-Trinder method), HDL- cholesterol by phosphotungstic acid method [5] , Total cholesterol by glucose oxidase and peroxidase (CHOD-POD) method [6,7] , VLDL-C and LDL-C were calculated by Friedewald WT formula [8] . Serum Glutathione peroxidase expressed in unit/gm of hemoglobin [9] and serum selenium estimated by atomic absorption spectrophotometery.
Statistical significance was calculated by applying student‘t’ test on subjects with and without CAD groups. P < 0.01 and P < 0.001 was taken as significant and P> 0.05 as non significant.
Table shows age and sex distribution in AMI. There are 03 male patients in the age group of 30-39 yrs, 09 male and 03 female in the age of 40-49yrs.15 male and 01 female in between age group of 50-59 yrs and 03 male and 02 female in age group of 60 yrs and above.
Table shows age and sex distribution in controls. There are 04 male in the age group of 30-39 yrs, 12 male and 01 female in the age of 40-49yrs.10 male and 03 female in between age group of 50-59 yrs and 03 male and 03 female in age group of 60 yrs and above.
(See [Table-3] )
Table shows significantly high serum levels of T-Cholesterol, VLDL, LDL-Cholesterol and triglycerides in AMI patients compared with controls with P < 0.001 and inverse relationship with HDL-Cholesterol, Serum GSH-PX and serum selenium and AMI patients with P < 0.001.
The oxygen derived free radicals are important mediators of oxidation of lipoproteins lead to progression of atherosclerosis and thrombosis results in myocardial tissue damage [10] . In myocardial infarction not only is the oxidative stress more but initial defense system against free radical is also suppressed [11] .
In ischemic heart disease (IHD), the appropriate prooxidant and antioxidant balance can be shifted towards pro-oxidants when the oxidant species is increased greatly. The major antioxidant enzyme selenium containing GSH-PX provides major removal of free radicals. Lipid peroxides and oxygen metabolites from heart [12] . The selenium could be protective against formation of MDA, a product of peroxidative tissue damage. The biological tissue contains variety of antioxidant including dismutase, catalase, glutathione peroxidase, thiol compounds and vitamins which can protect the cell and its membrane against peroxidative deterioration [13] .
In our study we found significantly low levels of GSH-PX in AMI patients as compared with controls [Table-3] . Our results are in accordance with several earlier workers [14,15] .
Konukoghu D et al [16] also reported that erythrocyte antioxidant GSH-PX was significantly low in AMI patients than controls (P<0.001) Whereas Ferrari et al [17] were not able to determine any changes in GSH-PX enzyme in heart tissue during iscaemia and reperfusion process. Low levels of GSH-PX in IHD may be because of its utilization in free radicals produced by lipid peroxidation [18] .
Because biological function of GSH-PX system is to prevent initiation of peroxidation of membrane lipid. Decrease in the level of GSH-PX in the present study [Table-3] might de due to its utilization in scavenging free radicals produced in lipid peroxidation in myocardial infarction.
As discussed earlier, lipid peroxides have been implicated in the initiation of coronary atherosclerosis and in order for glutathione peroxidase to be able to counteract the adverse effect of peroxide; sufficient amount of selenium must be available for formation of enzymes. The mechanism of action of this enzyme requires the presence of selenocysteinne in the active site [19] .
In present study, we observed [Table-3] significantly low serum selenium concentration in AMI cases compared with healthy controls. Our results maintain a fair correlation with findings of many workers [3,15,18,20] .
Hoffman A. [21] suggested that high oxidant stress present either before or after the event and findings indicates low selenium level present before infarction. They hypothesized that in selenium deficient state, there is decreased in GSH-PX activity. Selenium deficiency is because of dietary, metabolic, genetic influences. It is thus conceivable that under pathological condition an even higher concentration of selenium supply is required for adequate activity of GSH-PX.
We found positive correlation in between serum TC, TG, VLDL and LDL and AMI whereas, negative relationship between HDL-C and AMI cases, Serum lipid parameters are the well established risk factors for the Coronary artery disease [22,3] .
The evidence presented here indeed confirms that selenium is a strong antioxidant and when lacking, the arterial intima is prone to get oxidative damage. Selenium also play role in stabilization and in repair of damaged myocardial cell membrane as well as maintenance of normal function of cell.
Adequate selenium can reduce the range of myocardial infarct, increases the blood flow of coronary artery, and better micro vascular circulation and thus in short protect arteries from peroxidation and thus can prevent atherosclerosis and so the incidences of CAD development.
So, the estimation of serum selenium and glutathione peroxidase might be used to judge the antioxidant defense system in CAD patients and lipid parameters can help in prediction of risk of coronary artery disease.
[1] Raymann M.P. (2000) Lancet 356:233-41.2. www.heart.problems.net/, dt 2010-01-11.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
[2] Motghare K.S., Bhutey A. et al. (2001) Indian J. Clin Biochm, 16 (2): 213-215.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
[3] Mc Gowan M.W. (1983) Clin Chemistry, 29: 538-42 and Fossati P. (1969), Ann Clin Biochem. 6:24.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
[4] Burstin M., Scholnik H.R., Morfin R. (1970) J. Lipid Research 11: 583-94.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
[5] Richmond W. (1973) Clin. Chem.: 19 (12): 1350-56.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
[6] Allain C.C., Lucy S., Poon Paul C. and Fu et al. (1974) Clin Chem. 20 (4): 470-475.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
[7] Friedewald W.T., Levy R.I., Fredrickson D.S. (1972) Clin. Chem. 18 (6): 499-502.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
[8] Paglia E., Valentine E. (1967) J. Lab. Clin. Med, 1967, 70: 158.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
[9] Tramber M.G. and Kaylen H.K. (1980) Proc. Natl. Acad Sci; vol 77: 5466-5470.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
[10] Chandra M., Chandra N., Agrawal R. (1994) International J. Of Cardiology: 43: 121-25.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
[11] McCay P.B., Gibson D.D. etal. (1976) Biochem. Biophysics, Acta 431:459.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
[12] Merson F.Z., Kangan V.E. (1982) Basic Res Cardiol, 77; 465.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
[13] Gromadizinska J., Sklodowska M. (1990) JAMA, Feb; 263 (7): 949-950.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
[14] Gemma F.M., Ana N.A., Roberto P.B. etal (2006) The American J. Clin. Nutr. Oct, Vol 84 (4): 762-773.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
[15] Konukoglu D,. Akcay T. (1998) Clin. Biochem, 1998 Nov; 31 (8): 667-671.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
[16] Ferrari J. (1990) Lab Invest. 62: 670.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
[17] Salonen J.T., Salonen R., Puska P. (1985) Am. J. Cardiol. 56: 226-231.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
[18] Yegin H., Aliciguzel, Deger N. (1997) Jpn. Heart J, Nov; 38 (6): 793-798.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
[19] Kardinall A.F. et al. (1997) Am. J. Epidemiol. 145: 373-9.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
[20] Hoffman A., Kok F.J., Wittenman J. C. (1989) JAMA, Feb, 261 (8); 1161-1164.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
[21] Whayne T.F., Alaupovic P., Curry M.D. etal. (1981) Atherosclerosis, Jun; 39 (3): 411-24.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
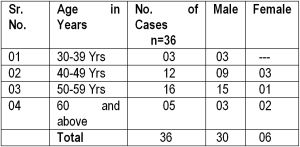 | Table 1- Age-sex distribution in AMI cases (n=36) |
 | Table 2- Age-sex distribution in healthy controls (n=36) |
 | Table 3- Biochemical Parameters in AMI Patients and matched controls |