ISSN : 0976-5530
EISSN : 0976-5549

VIDYULATA SALUNKHE1*, SUTRAWE A.2, RAJESH GOEL3, PRATAP JADHAV4
1MGM Institute of Health Sciences, MGM Campus, Sector 18, Kamothe, Navi Mumbai-410209, India
2MGM Institute of Health Sciences, MGM Campus, Sector 18, Kamothe, Navi Mumbai-410209, India
3MGM Institute of Health Sciences, MGM Campus, Sector 18, Kamothe, Navi Mumbai-410209, India
4MGM Institute of Health Sciences, MGM Campus, Sector 18, Kamothe, Navi Mumbai-410209, India
* Corresponding Author : s.vidyu@gmail.com
Received : 17-04-2011 Accepted : 18-05-2011 Published : 05-09-2011
Volume : 2 Issue : 1 Pages : 14 - 19
Int J Med Clin Res 2.1 (2011):14-19
DOI : http://dx.doi.org/10.9735/0976-5530.2.1.14-19
Conflict of Interest : None declared
The adolescence is phase of rapid growth and development where there is great deal of change taking place like physically, socially and emotionally. The major causes of death, disease and disability for young people have been identified as vehicular accident, suicide and unintentional injuries. But this is just a tip of ice berg, major health hazards like chronic illness and diseases are commonly caused by exposure to risk factors long before the onset of illness. It is the behavior pattern that is established during adolescence period which makes individuals susceptible to a number of illnesses that develop later in life.
Adolescent Health, smoking, alcohol, sexual, unhealthy dietary, physical, psychological.
The study was a cross-sectional study of the subject population. The units of the study were 17-19 years old adolescents studying in various colleges in Navi Mumbai. For the purpose of study; city was divided into 3 divisions. All the colleges in the region were included in the sampling frame. The questioner was developed with collection of existing survey [1] and discussion with health professionals. The questionnaire was piloted in a college among 17-19 years students. Structured and planned questioner was given to individuals and reliability of questioner was tested, which was found to be 97%. The same questioner was used in main study.
A multi stage sampling design was used to draw a representative sample of first year students of Colleges. The first stage was selection of six colleges by random sampling. In the selected colleges, one section from each class was randomly chosen. All students in the selected classes were present on the days of the survey, were eligible to participate, allowing for anonymous and voluntary participation. Written permission and consent from the principals was obtained prior to conducting the study in their colleges.
Objective: To identify the most common health risks amongst college-going adolescents in Navi Mumbai and establish the need of Adolescent clinics.
Study Design: Cross-sectional study.
Setting: Six colleges in Navi Mumbai.
Participants: Three hundred and seventeen adolescents aged 17-19 years. One hundred and ninety (59.9%) were females and one hundred twenty-seven (40.1%) were males.
Statistical analysis was performed using the Statistical Package for Social Sciences (SPSS 16). Data are presented as frequencies, means, and proportion. The Chi-square test was used to compare proportions in and between groups. Statistical significance was set at 5% & Likert’s scale was used to rank quantitative data wherever necessary e.g. Mental health, eating habits and behavior section. Adolescence is defined by WHO as the age group of 10− 19 years. Adolescents constituted 22.8% of the population in India. Adolescence is filled with challenging new experiences and for most adolescents it is a time of unparalleled potential and creative energy. At that age, they begin to probe more deeply to discover their individual identity and sort out values and beliefs in their quest for a clearer sense of self. Implementation of preventive and health promotion services is very efficient at this stage of the human life cycle. The present study covered important health risk behaviors among adolescents. This study was carried out with the purpose of finding out the prevalence of various health risk behaviors among the college going adolescents in Navi Mumbai. We also tried to find out association, if any, between health and socio-economic status of the adolescents.
Cigarette smoking is the major known cause of non-communicable diseases, such as cancer and cardiovascular diseases [2] . In same way, alcohol is also a known leading cause of death in later time of life. Developing countries are now witnessing an increase in consumption pattern. In India, the most susceptible time for substance abuse is during adolescence. Hence, there is an urgent need to curb substance abuse among youth. This study was conducted to estimate the prevalence of substance abuse among adolescents of Navi Mumbai.
In our study prevalence of smoking among males was found to be 19.7% and among females was 3.2%. Percentage of males in this study is higher than that reported by other study [3] . The difference between males and females is significant, (P<0.000) [4] . Among smokers 51.6% of adolescent started smoking in the age group of 17 to 18 years.9.6% adolescents gave the history of initiation of smoking before the age of 10 years. Among the smokers 45.1% were smoking more than 10 cigarettes per week and 12.9% were smoking more than 20 cigarettes per week. Prevalence of smoking increases with their socio economic status (14.6% of upper class whereas 4.3% in lower middle class). 17.4% of adolescents admitted to drinking alcohol out of which 24.6%% were male and 12.6% were female. The percentage difference between male and female is less as compared to other studies done. 8.5% adolescent gave history of their initiation of alcohol before the age of 15 years. 10.9% drink alcohol weekly, 16.4% once a month and others occasionally. Over all there is no significance difference between males and females regarding their drinking habits. Friends contributed 77.1% and family 23% as source of initiation of substance abuse which is much higher than the findings of other study [5] . Admiration by peer (35.4%) was most common reason for continuation of substance abuse. Prevalence of drinking alcohol increases with socio economic status (46.3% of upper class where as 21.7% of lower class). In terms of source of knowledge regarding substance abuse, media (52.6%) was found to be commonest source and other sources were friends (41.9%), teachers (19.3%) and doctors (32.2%).One important finding here is that friends or peer group are the one who not only are the reasons for continuation of substance abuse but also are key source for awareness regarding harmful effects of substance. 83.9% believes substance abuse is bad for health. Major sources of information about harmful effect of substance abuse were media (52.6%), friends(41.9%), school teachers (19.3%) and doctors (32.2%).
Adolescents suffer from psychosocial problems at one time or the other during their growing period. To know the psychosocial problems among adolescents, this section is divided into behavioral problems, psychological problems, stress, suicidal tendencies and knowledge about redressal agencies.
In our study, behavioral difficulties were found to be more in males (6.7%) as compared to females (2.6%). The difference between males and females is significant, P<0.002. 7.6% of adolescents said they are not able to get along with their family members.
In our study, behavioral difficulties were found to be more in males (6.7%) as compared to females (2.6%). The difference between males and females is significant, P<0.002. 7.6% of adolescents said they are not able to get along with their family members. 7% are not able to get along with their friends and other people. 8.6% said they are not doing well in their studies. 11% are not allowed to do things as they wanted in their daily life. One more significant finding is that females have significantly more close friends in comparison to males. This may be because of females are more forth coming about their problems and more social in general.
The prevalence of the psychosocial problems was 19.2% among adolescents. The most common problem was educational difficulties found in 34.1% of the study population. 29% said they have trouble falling asleep or staying asleep. 35% said they cry a lot which comprises of 32.2% of females and 11.8% of males of total adolescents under study. 28.6% said they are easily irritable in nature. 31.7% gets easily in arguments or fights.
16.6% say they are under stress and among these 38.8% feel lonely, 20.9% are depressed about life in general.
16.8% have thought of suicide out of which 9.2% have seriously thought to end their life. 5.4% have attempted suicide with no significant difference between male 7 (5.5%) and female 10 (5.3%).
Adolescent said whenever they feel depressed; they would like to discuss their problem with (72.4%) friends, (16.9%) siblings, (2.2%) doctors, (19 %) themselves. The concept of adolescent clinic is unheard by majority of youth (95.6%).
Higher prevalence of the psychological problems in Upper Social economic class (40.3%) as compared to (.3%) in lower socio economics class was observed which is in contrary to other researches [6,7] .
Inadequate nutrition in adolescence can potentially retard their growth and can make them easily prone to many communicational and non- communicational diseases. Almost half of the population under study was non-vegetarian and remaining half is vegetarian. Among the vegetarian 19.6% population have occasional eggs. 39.4% of adolescents say they eat vegetables daily and 34.7% eat fresh fruits daily. 88.5% of adolescent under this study, say they pay attention to see that their diet is healthy. 17.4% say they have fasted to lose weight. Because some or other reason 11% adolescents eat food outside daily and rest of them have their meals at home. This may be due to the fact that these adolescents have migrated to this city for educational purpose.
10.4% of adolescent say they have missed college during last year because of dental problems. In this 14.7% of females and 3.9% of males missed their college because of dental problem. The proportion of females who missed their college because of dental problems was found to be significantly (P<0.001) more than in males. 24.9% adolescent say they visit dentist regularly out of which 30% are females and 17.3% are males.
We were interested in knowing how exactly today youth keeps themselves busy during their free time.
In this contest we asked them to pin point the exact way of spending their free time. 44% of youth (52.7% of females and 33.9% of males) engages themselves in watching TV during free time. 15.6% watch TV or play games on computer for more than 3 hour a day. 23.5% of adolescents (42.6% of males and 11.1% females) are involved in sports. 54.6% say they are not at all involved in any physical activity like sports.
25% adolescents have normal BMI and 1% adolescents are over-weight. 74% are under weight out of which 85.3% are females and 58.2% are males. The proportion of underweight females was significantly (P<0.000) more than underweight males under study. Percentage of underweight adolescent in this study is higher than in other studies [8,9] .
This study was undertaken among college students to assess the level of knowledge on the existence, mode of transmission and prevention of acquired immunodeficiency syndrome (AIDS) and also to elicit the history of sexual exposure. 88.6% of adolescents are aware about HIV/AIDS. 43.2% of adolescents had knowledge of all the modes of transmission of HIV. 91.7% of the subjects were aware that HIV/AIDS could be transmitted through sexually, 68.5% through infected injection, 62.4% from infected mother to baby. 67.8% think using condom during intercourse can prevent HIV. 97.9% say they will search on internet/magazines if they have some sexual or reproductive health problem and 58.7% say they will consult a doctor, 23.5% will ask friends and 4.9% will wait to heal itself. 46.7% don’t have knowledge about emergency contraceptive with no significant difference between female and male observed. 9.8% of adolescent had knowledge of all three methods of contraception i.e. barrier, pills and rhythm method. When asked ,if they will sit in the same class with HIV positive student, 41.8% adolescent said yes and remaining were not willing to sit (37.7%) or not sure (20.6%). 8.5% have had sexual intercourse out of which 13.4% are males and 5.3% are females. The difference being statistically significant which is similar to the findings of other study [10] . 3.1% male say they had gotten some one pregnant ever and 1.1% females said they have been pregnant at some point of time in life. 1.1% females say they have got abortion done. Males are significantly (p<.000) more involved in high−risk sexual behavior than females.
Injuries are a major cause of death and disability among the adolescents in the world. These include unintentional injuries such as involvement in road traffic accidents, injuries resulting from interpersonal violence such as involvement in physical fights. This study was carried out with the purpose to find out the prevalence of various health risk behaviors among the college-going adolescents. The questionnaire was made with the help of existing survey [11] and discussion with health professionals.
Among the study participants, 12.6% reported having carried a weapon in past 30 days (no significant difference between male and female) which shows now more females are carrying weapons with them , which is significantly more then as shown in older studies [12] . 9.5% of adolescents had threatened or injured someone with a weapon in past 12 months. 35.8% males and 18.5% females reported having being involved in a physical fight in last year, where difference between male and female was significant (p<0.000). Across the globe, about one-third to one-half of the adolescent students report involvement in physical fights [13,14] and the present findings fit the trend. 14% reported having received an injury in a physical fight, which was serious enough to require medical attention, during the last 12 months. 36.7% adolescents feel unsafe most of the time out of which 54.8% are males and 24.7% are females. The difference between males and females is significant, P<0.000. 45.3% males and 25.3% females say their parent knows a little about what they do in their free time.17.4% of adolescents feel they are alone at home most of the time, out of which 21.4% are males (which is significantly more p<0.003) and 14.7% are females. By looking at all these figures most of adolescents feel unsafe and less secure. These figures also indicate the growing impatiens and trend towards unnecessary fights, arguments and short temperedness.
Prevalence of smoking and alcohol was 9.8% and 17.4% respectively among study population. Majority of adolescents (54.6%) have sedentary life style. 74% of adolescents were underweight. Among underweight students, 85.3% were females and 58.2% were males. The prevalence of overall psychosocial problems was 19.2% among adolescents. 20.9% adolescent were depressed about life in general.17.4% feel alone at home most of the time, out of which 21.4% are males. 9.2% seriously considered attempting suicide.14.8% adolescents are eating fast food almost daily. 46.7% adolescents don’t have knowledge about emergency contraceptive.12.6% adolescent carries weapon to college. 35.8% males and 18.5% females reported having being involved in a physical fight in last year.
The present study has highlighted the emerging problems among adolescents. Many of problems identified are detrimental to health and potentially cause harm: both immediately an over a period of time (long term effects).
The high prevalence of smoking and intake of alcohol points out the necessity for a comprehensive strategy to curb the problem. Hence, a very pragmatic approach to containing the problem would be improved information education communication activities especially directed toward adolescents and through media. Another problem is psychological ill health of adolescents. Poor mental health awareness, limited school and other community−based services combines to make adolescents an underserved population in our country. The combination of ignored psychosocial problems and the lack of mental health services in our country amplify the risk of precipitating academic underachievement and rising Delinquent behavior in adolescents. There is need to raise public awareness about the prevalence of these often hidden emotional disorders in Indian adolescents. Based on the findings of this study it is recommended that consumption of Junk food and snacking in between the meals should be avoided by children. Sedentary life style should be discouraged. Increase physical activity like playing outdoor games, cycling should be encouraged in children especially in females. Health education should be given to parents, teachers and children regarding dietary habit and sedentary life style (school based intervention).
Also a section of adolescents, though very small in number, also indulged in high−risk sexual behavior. IEC programs should be undertaken with regard to HIV/ AIDS, safe sex and avoidance of high−risk sexual behavior in schools and colleges to increase the awareness of adolescents. Scientific information regarding reproductive and sexual health should be included in the school curriculum to build up responsible sexual behavior among the students during adolescence as well as adulthood. Further studies are needed to cover the groups of adolescents who are out of school or college, as the prevalence of health risk behaviors is likely to be higher among such adolescents. Moreover, qualitative research methods like focused group discussions can be utilized in further studies to have in-depth analysis of the reasons for violent behaviors amongst school- and college-going adolescents. There is a need to reinforce positive health behaviors, for example, exercise and good nutrition while discouraging potentially health-risk behaviors, for example, violence and unsafe driving. It is strongly recommended that, there is need of Adolescent Clinics in society where adolescents can easily go and discus their problems freely with health professionals.
[1] Warren R. Stanton, Michelle Willis and Kevin P. Balanda (2000) Health education research, 15(2), 1081–190.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
[2] Rudatsikira E., Dondog J., Siziya S., Muula A.S. Singapore Medical Journal; 49 (1):57-62.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
[3] Rekha P Shenoy, Prashanth K Shenai1, Ganesh Shenoy Panchmal, Shashidhar M Kotian (2010) Indian Journal of Community Medicine, 35 (3), 433-435.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
[4] Lisa Sarangi, Himanshu P Acharya, Om P Panigrahi (2008) Indian Journal of Community Medicine, 33(4), 265-267.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
[5] Naskar N.N., Ray M., Bhattacharya S.K. (2004) Indian Journal of Community Medicine, 29, 69−71.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
[6] Anita, Gaur D.R., Vohra A.K., Subash S., Khurana H. (2003) Indian Journal of Community Medicine, 28, 133−7.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
[7] Anees Ahmad, Najam Khalique, Zulfi A Khan, Ali Amir (July 2007) Indian Journal of Community Medicine, 32 (3), 219-221.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
[8] Shahabuddin A.K., Talukder K., Talukder M.K., Hassan M., Seal A., Rahman Q. (2000) Indian Journal of Pediatrics , 67(2), 93-98.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
[9] Aparajita Dasgupta, Arindam Butt, Tushar Kanti Saha, Gandhari Basu, Amitava Chattopadhyay, Anindya Mukherjee (2010) Indian Journal of Community Medicine, 35(2), 276-279.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
[10] Arindam Chakrovarty, Saswati Nandy, Rabindranath Roy, Bhaswati Sengupta, Sukanta Chatterjee, Ramendra Narayan Chaudhuri (2007) Indian Journal of Community Medicine, 32(3), 228-229.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
[11] Rahul Sharma, Vijay L Grover, Sanjay Chaturvedi (2008) Indian journal of community medicine, 33 (2), 85-88.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
[12] Orpinas P.K., Basen-Engquist K., Grunbaum J.A., Parcel G.S. (1995) Journal of Adolescent Health, 16(3), 216-25.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
[13] Vanderschmidt H.F., Lang J.M., Knight-Williams V., Vandeschmidt G.F. (1993) Journal of Adolescent Health, 14, 282-8.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
[14] Ruangkanchanasetr S., Plitponkarnpim A., Hetrakul P., Kongsakon R. (2005) Journal of Adolescent Health, 36,227-35.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
 | Fig. 1- |
 | Fig. 2- |
 | Fig. 3- Distribution of students according to awareness about transmission of AIDs (acquired immunodeficiency syndrome) |
 | Table 1- Frequency of drinking alcohol |
 | Table 2- Distribution based on reasons for continuation of substance abuse |
 | Table 3- Factors responsible for stress among adolescents |
 | Table 4- Dietary habits |
 | Table 5- The frequency of consumption of fast food in a week |
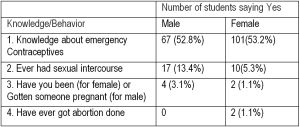 | Table 6- Sexual behavior of adolescents under study |
 | Table 7- Prevalence of risk behaviors related with inter-personal violence among the respondents |