ISSN : 0976-5530
EISSN : 0976-5549

HARITHA KUMARI N.1*, MINI MOL P.2, NAZMEEN SILOTRY3
1Department of Anatomy, MGM Medical College, Sector-18, Kamothe, Navi Mumbai, India.
2Department of Anatomy, MGM School of Biomedical Sciences, Sector-18, Kamothe, Navi Mumbai, India.
3Department of Anatomy, MGM Medical College, Sector-18, Kamothe, Navi Mumbai, India.
* Corresponding Author : haritha_anat@yahoo.com
Received : 16-02-2012 Accepted : 09-03-2012 Published : 29-03-2012
Volume : 3 Issue : 3 Pages : 136 - 139
Int J Med Clin Res 3.3 (2012):136-139
DOI : http://dx.doi.org/10.9735/0976-5530.3.3.136-139
Conflict of Interest : None declared
Acknowledgements/Funding : We cordially thank our Head of the department, Dr. Aruna Mukherjee, for her extensive support and guidance throughout the study period and we also thank Dr.Narshetty, Dean, MGM Medical College for his great support and permitting us to perform this study
Aim and Objectives: To measure, calculate, find out variations and finally compare the pattern of talar articular facets of different human calcanei. Materials and Methods: 50 adult human calcanei were obtained irrespective of age and sex and evaluated one by one. Three types of calcaneus that has distinct talar facets as Types A, B and C and sub types were defined. Results: The study reveals the following results; Out of 50 calcanei 13 were of Type A (26%) 37 were of Type B (74%) and None were of Type C. The mean intersecting angle of Type A calcaneum is 121.50 and The mean intersecting angle of Type B calcaneum is 151.60 Conclusion: This study reveals that the talar facet configuration of calcanei and angle between the anterior and middle facet influences the stability of the subtalar joint.
Calcaneus, facets, subtalar joint.
The calcaneus is the longest and the largest of the tarsal bone. It articulates with the overlying talus to form the talocalcaneal joint which together with talocalcaneonavicular joint are clinically referred to as the subtalar joint [1] , where the important movements of inversion and eversion of the foot occur.
There are three facets over superior surface of talocalcaneal joint: anterior talar facet, middle talar facet and posterior talar facet [2] . The middle third of the superior surface of the calcaneum carries the posterior talar facet for the articulation with the body of the talus. In most textbooks of Anatomy descriptions of the posterior talar facet on the middle third of the dorsal surface of the calcaneus are similar [3-5] . However, descriptions of the facet for the head of the talus are at variance. In the anterior third of the calcaneus, distal and medial to the sulcus calcanei, an articular area covers the sustentaculum tali, this facet articulates with the head of the talus, and may be divided in about half the cases by a non articular zone creating middle and anterior talar facets, the incidence of which varies with race and sex [6] .
Changes in the human foot associated with the evolution of bipedalism involved the elevation of the calcaneus which increased the inclination of the subtalar joint axis to approximately 420. This elevation was crucial for the formation of the longitudinal arch. The sustentaculum tali is at the 'apex' of the longitudinal arch and thus occupies a key position in the subtalar joint. It functions as a bracket that supports the talar head and is responsible for transmission of force towards the lateral arch [7-9] .
Variations in the articular facets of the sustentaculum tali have been described by many authors. Although these researchers use slightly different classificatory schemes, 3 distinct facet types are generally recognised:
1. long continuous facet
2. separate facets and
3. Only one continuous facet
These facet configurations are present in fetal calcanei and are not developmental responses to physical activities [9] .
Most researchers view these differences in facet configuration as anatomical variations of no functional significance. Bruckner [10] in contrast, argues that the 2-facet configuration is more stable than the others. The 2-facet configuration is typically associated with a higher angled subtalar joint axis and a sharper intersecting angle, i.e. “Critical angle of Gissane†of the anterior and medial facets [10] . These characteristics, in conjunction with the posterior talocalcaneal facet, cause the talus to sit on an 'osseous tripod' and prevent excess motion of the talar head. A 2-facet configuration is more stable, there should be less evidence of pathological changes associated with this configuration.Unstable joints are more likely to suffer trauma, accidents, or other biomechanical stress as a result of uneven weight distribution [6-8] .
Using parameters such as degree of separation, fusion and shape, some researches have described types and preponderance of articular facets. Morphometric values of calcanei are important for the science of anatomy, treatment and diagnosis procedures on orthopedic surgery, kinesiology, physical treatment and rehabilitation sections. The racial and individual differences of the anatomic construction of the calcanei play a key role on static and kinetic dynamic on the foot. During the treatment period of the congenital club foot, talocalcaneal coalition, severe pronation cases, valgus deformities, subtalar instability and development of subtalar implants talus-calcaneus with each other and other bones of foot should well defined [9,11,12] . Calcaneal lengthening osteotomy, as popularized by Mosca, is extra-articular, with its site being the interval between the anterior and middle calcaneal facets. For individuals without a distinct anterior and middle facet, the subtalar joint must be violated to perform this operation [13] . The detailed calcaneal anatomy shall facilitate the alternatives of treatment procedures.
Fifty adult human calcanei were obtained from the Department of Anatomy, MGM Medical College, Kamothe, Navi Mumbai and MGM Medical college, Aurangabad irrespective of age and sex and evaluated one by one. The study was carried with naked eyes and hand lens in broad day light and distance between the facets were measured with a vernier calliper.
According to Mujde.U, et al [2] , three types of calcaneii that has distinct talar facets as Types A, B and C and sub types were defined.
On calcaneus, two anterior articular facets.
Type A is divided into following four subtypes [Fig-1]
• A1: the distance between anterior and middle talar facets was less than 2Â mm.
• A2: the distance between anterior and middle talar facets was 2-5Â mm.
• A3: the distance between anterior and middle talar facets was more than 5Â mm.
• A4: there was only one joint facet, named as anterior talar facet.
The A1, A2 & A3 types have three joint facets while A4 has two.
Single anterior and middle articular facets fused.
Type B is again subdivided into [Fig-2]
• Type B1: the separation between these two joint facets was not completed. The shape of facet joint was constricted (antero-middle joint facets were constricted).
• Type B2: there was no separation between these two joint facets. There was only one wide smooth facet (unconstricted).
An anterior and posterior articular confluent facet i.e. there is one joint facet [Fig-3] angle formed by the intersection of the medial and anterior facets of the sustentaculum tali, was determined using the following procedure. The calcaneus was placed on its medial side on a piece of paper so that the medial border of the sustentaculum tali facets contacted the paper and the planes of the facets were perpendicular to the surface of the paper. The contour of the facets was traced with a pencil and the angle measured with a protractor [Fig-4] . Repeated observations made on the same series of bones indicated that the average error of this measurement is about 2° [13] .
The presence of lipping and osteophytes was determined by visual inspection of the articular surfaces.
The study reveals the following results; [Table-1] , [Table-2] , [Table-3] , [Table-4] .
The joint facets on calcanei which articulate with talus show variations with race and sex. In textbooks, anterior and posterior facets are mentioned separately while the middle one is defined as the continuation of the anterior facet. Although it is necessary to define and appreciate these differences for medical science to make accurate diagnosis and the treatment, there is no detailed knowledge indicating these differences. It is well known that the treatment choices of the complex foot deformity are osteotomy and relaxation of the soft tissue to obtain a painless and functional foot [9,11,14,15,19] .
Our study on Indian population determined that only 13% among the 50 calcanei were of Type A i.e. with a distinct anterior and middle facet whereas 34 % of the calcaneum had Type B facet i.e. joined anterior and middle facet and none were of Type C i.e. single facet formed by joining of all the three facets. Our studies were similar to those of Bunning and Bannet’ s study on Indian race were Type A was 22%, Type B 78% and none was of Type C. It was also similar to studies conducted by Padmanabhan on Indian race and also with Campose and Pellico on Spanish population were the Type B facet was more compared to Type A facet but differ from the study done on European population were Type A facet was more i.e. 67% compared to Type B i.e. 33% and none was of Type C. Results of our study is similar to that of study by Gupta et al on Indian population except that Gupta et al detected 2% of Type C calacaneum among 401 samples studied.
The variations in the superior surface of the calcaneus enable the calcanei to be classified according to the number and disposition of the articular facet of the talus. In this study Type B (single anterior and middle facet fused) was 74% with mean intersecting angle of 151.60 and Type A (two anterior facet) 76% with mean intersecting angle of 121.50.
This study reveals that the talar facet configuration of calcanei and angle between the anterior and middle facet influences the stablility of the subtalar joint.
We cordially thank our Head of the department, Dr. Aruna Mukherjee, for her extensive support and guidance throughout the study period and we also thank Dr. Narshetty, Dean, MGM Medical College for his great support and permitting us to perform this study.
[1] Saadeh F.A., Fuad A.H., Mahmond S.M., Marwan E.E. (2000) Journal of Anatomical society of India, 49, 6-8.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
[2] Mujde Uygur, Funda Atamaz, Servet Celik, Yelda Pinar (2009) Archives of Orthopaedic & Trauma Surgery. 129(7), 909-914.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
[3] Breathnach A.S. (1965) J. & A. Churchill Ltd., 6th ed. 147.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
[4] Last R.J. (1970) The English Language Book Society and J. & A. Churchill Ltd., 4th ed., 341.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
[5] Warwick R., Williams P.L. (1973) Gray's Anatomy, 35th edition, Edinburgh: Longman Group Ltd, 377.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
[6] Kapandji I.A. (1970) The Physiology of the Joints, 2, Lower Limb. New York: Churchill Livingstone.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
[7] Harris N.H. (1983) The ankle and foot. In Postgraduate Textbook of Clinical Orthopaedics, 840-870.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
[8] Olson T.R., Seidel M.R. (1983) Foot and Ankle, 3, 322-341.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
[9] Banning P.S.C., Barnett C.H. (1965) Journal Anat., 99, 77-76.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
[10] Bruckner J. (1987) Journal of Orthopedic and Sports Physical therapy, 8, 489-494.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
[11] Ananthakrisnan D., Ching R., Tencer A., Hansen S.T., Sangeorzan B.J. (1999) J. Bone Joint Surg., 81(8), 1147-1154.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
[12] Dogan A., Albayrak M., Akman Y.E., Zorer G. (2006) Acta Orthop Traumatol Turc, 40(5), 356-366.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
[13] Francine Drayer-Verhagen (1993) J. Anat., 183, 631-634.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
[14] Csizy M., Buckley R., Tough S., Leighton R., Smith J., McCormack R., Pate G., Petrie D., Galpin R. (2003) J. Orthop. Trauma, 17(2), 106-112.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
[15] Dogan A., Albayrak M., Akman Y.E., Zorer G. (2006) Acta Orthop Traumatol Turc, 40(5), 356-366.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
[16] Giannini S., Ceccarelli F., Vannini F., Baldi E. (2003) Clin Orthop Relat Res, 411, 178-187.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
[17] Koshy S., Vettivel S., Selvaraj K.G. (2002) Forensic Sci Int, 129(3), 200-204.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
[18] Kwak Y.H., Park K.B., Park H.W., Kim H.W. (2008) Yonsei Med J., 49(1), 79-83.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
[19] Moore K.L., Dalley A.F. (2006) Clinically oriented anatomy, 5th edn edn. Lippincott Williams & Wilkins, Philadelphia, 570-571.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
[20] Oznur A., Komurcu M., Marangoz S., Tasatan E., Alparslan M., Atesalp A.S. (2007) Int Orthop. 478-482.
» CrossRef » Google Scholar » PubMed » DOAJ » CAS » Scopus
 | Fig. 1- Type A: On calcaneus, two anterior articular facets. |
 | Fig. 2- Type B: Single anterior and middle articular facets fused. |
 | Fig. 3- Single joint facet |
 | Fig. 4- Measuring Degrees of intersecting angles: (a) continuous facet configuration Mean angle 121.50; (b) 2-facet configuration Mean angle 151.60. |
 | Table 1- Showing different types of articular facets of calcanei |
 | Table 2- Showing the numbers and percentages of incidences of talar articular facets on calcaneum |
 | Table 3- Showing percentages and the degrees of intersecting angles of facet types. |
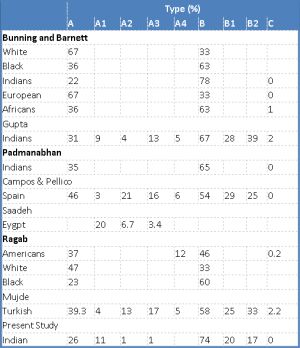 | Table 4- The comparison of results of the present study with those of the other researchers. |